


 Sign Out
Sign Out




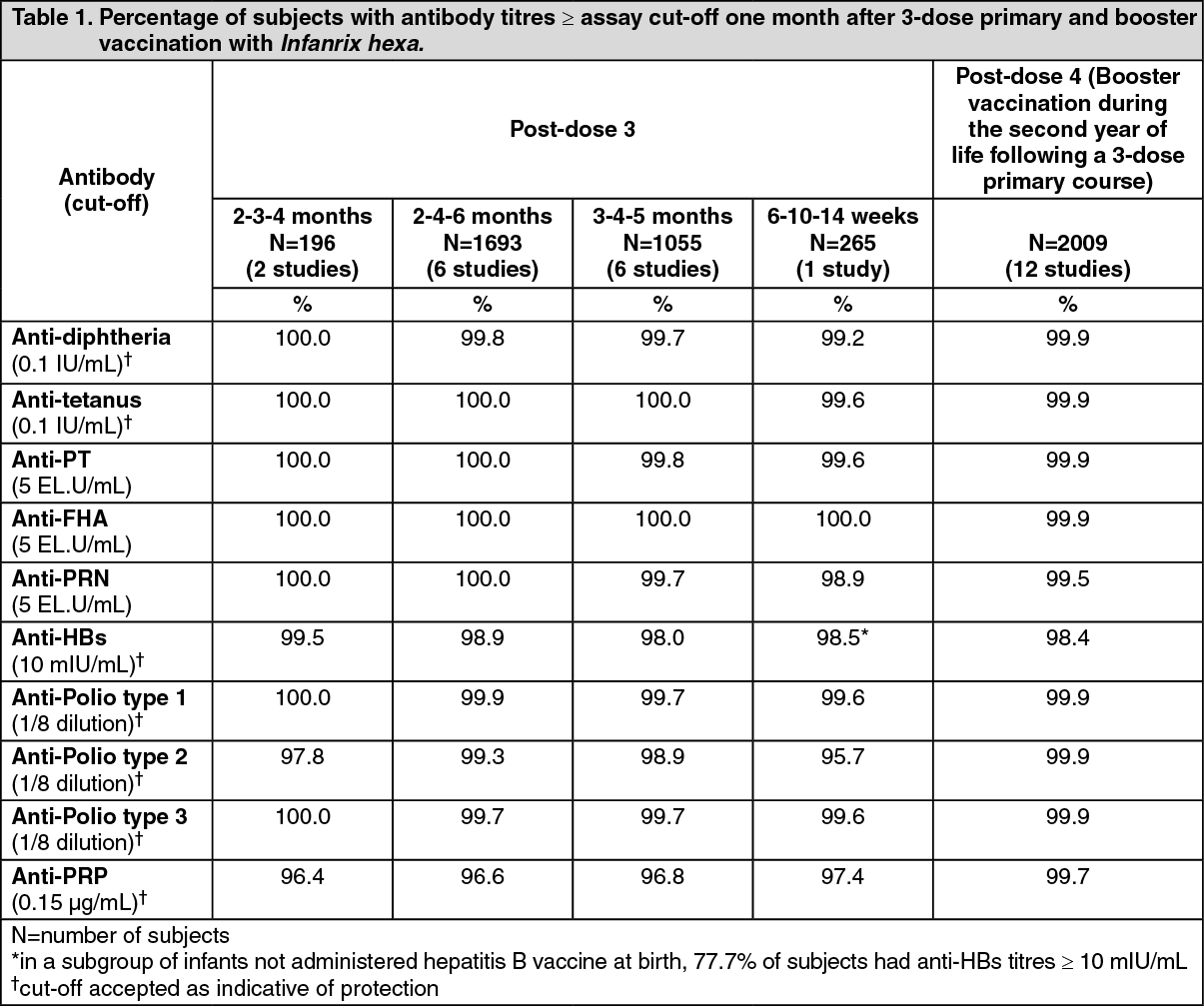
Pharmacology: Pharmacodynamics: Immunogenicity: The immunogenicity of Infanrix hexa has been evaluated in clinical studies from 6 weeks of age. The vaccine was assessed in 2-dose and 3-dose priming schedules, including the schedule for the Expanded Program on Immunisation, and as a booster dose. The results of these clinical studies are summarised in the tables as follows.
After a 3-dose primary vaccination schedule, at least 95.7% of infants had developed seroprotective or seropositive antibody levels against each of the vaccine antigens. After booster vaccination (post-dose 4), at least 98.4% of children had developed seroprotective or seropositive antibody levels against each of the vaccine antigens. (See Table 1.)
 Click on icon to see table/diagram/image
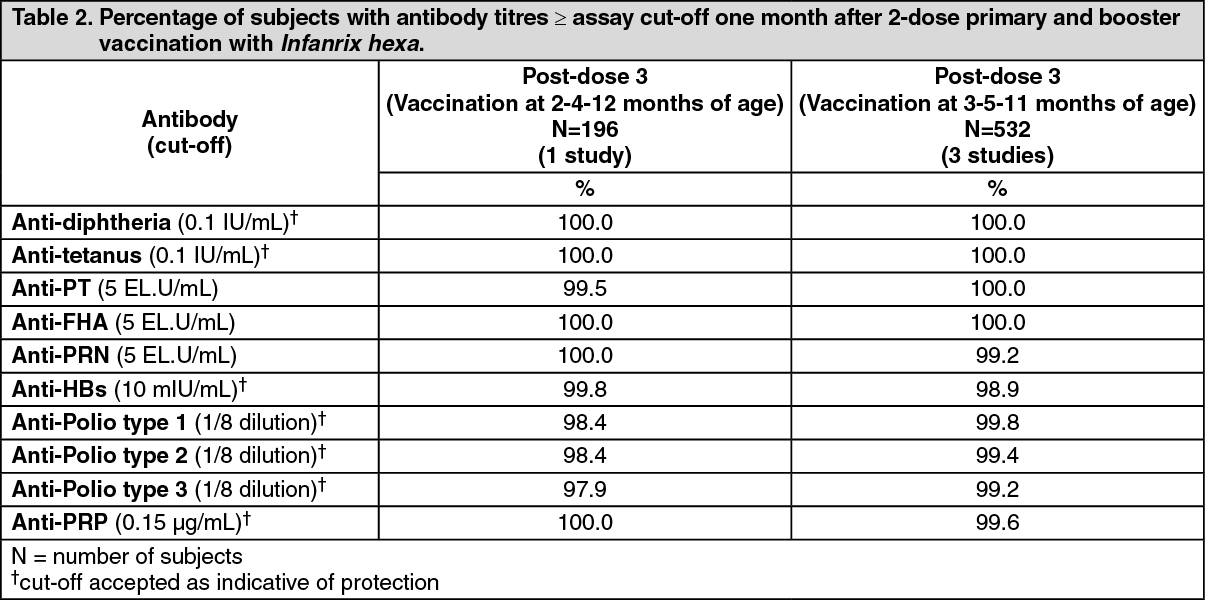
Click on icon to see table/diagram/imageAfter a complete vaccination according to a 2-dose primary and booster schedule with Infanrix hexa, at least 97.9% of the subjects had developed seroprotective or seropositive antibody levels against each of the vaccine antigens. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSerological correlates of protection have been established for diphtheria, tetanus, polio, Hepatitis B and Hib. For pertussis there is no serological correlate of protection. However, as the immune response to pertussis antigens following Infanrix hexa administration is equivalent to that of Infanrix (DTPa), the protective efficacy of the two vaccines is expected to be equivalent.
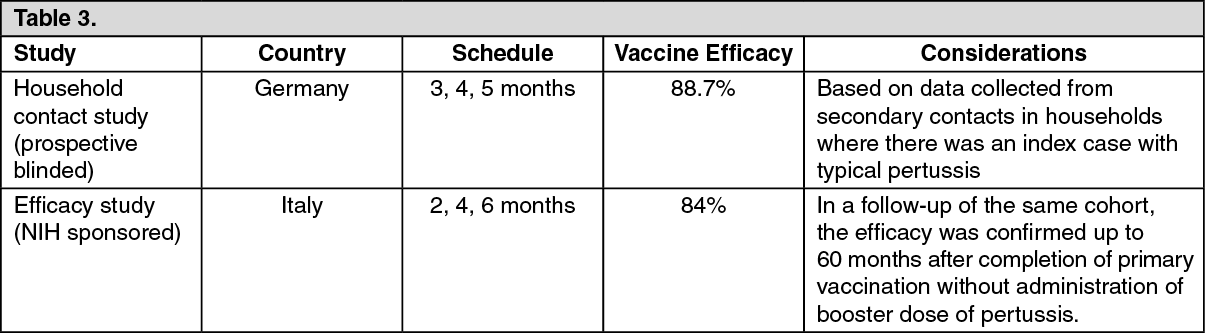
Efficacy in protecting against pertussis: The protective efficacy of the pertussis component of Infanrix (DTPa) against WHO-defined typical pertussis (≥ 21 days of paroxysmal cough) was demonstrated after 3-dose primary immunisation in the studies tabulated as follows: (see Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity in infants and toddlers born to mothers vaccinated with dTpa during pregnancy: Clinical data from more than 500 infants and toddlers did not show clinically relevant interference between maternal vaccination with Boostrix and the infant and toddler response to diphtheria, tetanus, hepatitis B, inactivated polio virus, Haemophilus influenzae type b or pneumococcal antigens. Although lower concentrations of antibodies against some pertussis antigens were observed post primary and post booster vaccination, 92.1-98.1% of subjects born to vaccinated mothers showed a booster response against all pertussis antigens. Current epidemiological data on pertussis disease do not suggest any clinical relevance of this immune interference.
Immunogenicity in preterm infants: The immunogenicity of Infanrix hexa was evaluated across three studies including approximately 300 preterm infants (born after a gestation period of 24 to 36 weeks) following a 3-dose primary vaccination course at 2, 4 and 6 months of age. The immunogenicity of a booster dose at 18 to 24 months of age was evaluated in approximately 200 preterm infants.
One month after primary vaccination at least 98.7% of subjects were seroprotected against diphtheria, tetanus and poliovirus types 1 and 2; at least 90.9% had seroprotective antibody levels against the hepatitis B, PRP and poliovirus type 3 antigens; and all subjects were seropositive for antibodies against FHA and PRN while 94.9% were seropositive for anti-PT antibodies.
One month after the booster dose at least 98.4% of subjects had seroprotective or seropositive antibody levels against each of the antigens except against PT (at least 96.8%) and hepatitis B (at least 88.7%). The response to the booster dose in terms of fold increases in antibody concentrations (15- to 235-fold), indicate that preterm infants were adequately primed for all the antigens of Infanrix hexa.
In a follow-up study, approximately 2.5 to 3 years after the booster dose, 85.3% of the children were still seroprotected against hepatitis B and at least 95.7% were seroprotected against the three poliovirus types and PRP.
Persistence of the immune response: The persistence of the immune response to a 3-dose primary and booster schedule with Infanrix hexa was evaluated in children 4-8 years of age. Protective immunity against the three poliovirus types and PRP was observed in at least 91.0% of children and against diphtheria and tetanus in at least 64.7% of children. At least 25.4% (anti-PT), 97.5% (anti-FHA) and 87.0% (anti-PRN) of children were seropositive against the pertussis components.
With regards to hepatitis B, seroprotective antibody concentrations following a 3-dose primary and booster schedule with Infanrix hexa have been shown to persist in ≥ 85% of subjects 4-5 years of age, in ≥72% of subjects 7-8 years of age, in ≥60% of subjects 12-13 years of age and in 53.7% of subjects 14-15 years of age. Additionally, following a 2-dose primary and booster schedule, seroprotective antibody concentrations against hepatitis B persisted in ≥ 48% of subjects 11-12 years of age.
Hepatitis B immunological memory was confirmed in children 4 to 15 years of age. These children had received Infanrix hexa as primary and booster vaccination in infancy, and when an additional dose of monovalent HBV vaccine was administered, protective immunity was observed in at least 93% of subjects.
Post-marketing experience: Results of long term follow-up in Sweden demonstrate that acellular pertussis vaccines are efficacious in infants when administered according to the 3 and 5 months primary vaccination schedule, with a booster dose administered at approximately 12 months. However, data indicate that protection against pertussis may be waning at 7-8 years of age. This suggests that a second booster dose of pertussis vaccine is warranted in children aged 5-7 years who have previously been vaccinated following this schedule.
The effectiveness of the Hib component of Infanrix hexa was investigated via an extensive post-marketing surveillance study conducted in Germany. Over a seven year follow-up period, the effectiveness of the Hib components of two hexavalent vaccines, of which one was Infanrix hexa, was 89.6% for a full primary series and 100% for a full primary series plus booster dose (irrespective of the Hib vaccine used for priming).
Infanrix hexa has been the principal Hib-containing vaccine available in Italy since 2006. The vaccine is administered at 3, 5 and 11 months of age and coverage has exceeded 95%. Hib disease has continued to be well controlled, with no more than three confirmed Hib cases reported annually between 2006 and 2011 in Italian children aged less than 5 years.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not required for vaccines.
Toxicology: Pre-clinical Safety Data: Preclinical data reveal no special hazard for humans based on conventional studies of safety, specific toxicity, repeated dose toxicity and compatibility of ingredients.